Dr. Lincoff was renowned for his detailed, colored-pencil retinal drawings of every patient. Photo courtesy Norah Lincoff, MD
Contributed by D. Jackson Coleman, MD
Harvey A. Lincoff, MD, was a founder of modern retinal detachment surgery. He was a professor of ophthalmology, Newhouse Clinical Scholar, and former director of retinal research at the New York Presbyterian Hospital--Weill Cornell Medical Center.
In the spring 2018 Retina Times, D. Jackson Coleman, MD, recalled, “In an illustrious retina career spanning more than 50 years, Harvey Lincoff developed enduring surgical techniques and instruments, including cryosurgery using liquid nitrogen to repair retinal detachments, the curved, spatula-shaped needles to help reduce accidental perforation during surgery, and the soft silicone sponge and balloon that bear his name.
“Principled, talented, and inventive, Harvey is best known for his detailed retinal drawings and for developing his Lincoff’s Rules for finding the retinal hole, which substantially improved surgical results.
“Harvey Lincoff was rewarded with most of the honors bestowed by ophthalmology societies, including the American Academy of Ophthalmology. Much of his work was done with Ingrid Kreissig, MD, his professional collaborator for 48 years. They wrote book chapters and papers,and lectured worldwide.
“He is a superb example of someone who exuded the true art and practice of medicine—seeing, doing, and teaching. Harvey was also a good man and true friend to many of us."
highlights
1953
Established transscleral buckling without drainage (Ernst Custodis)
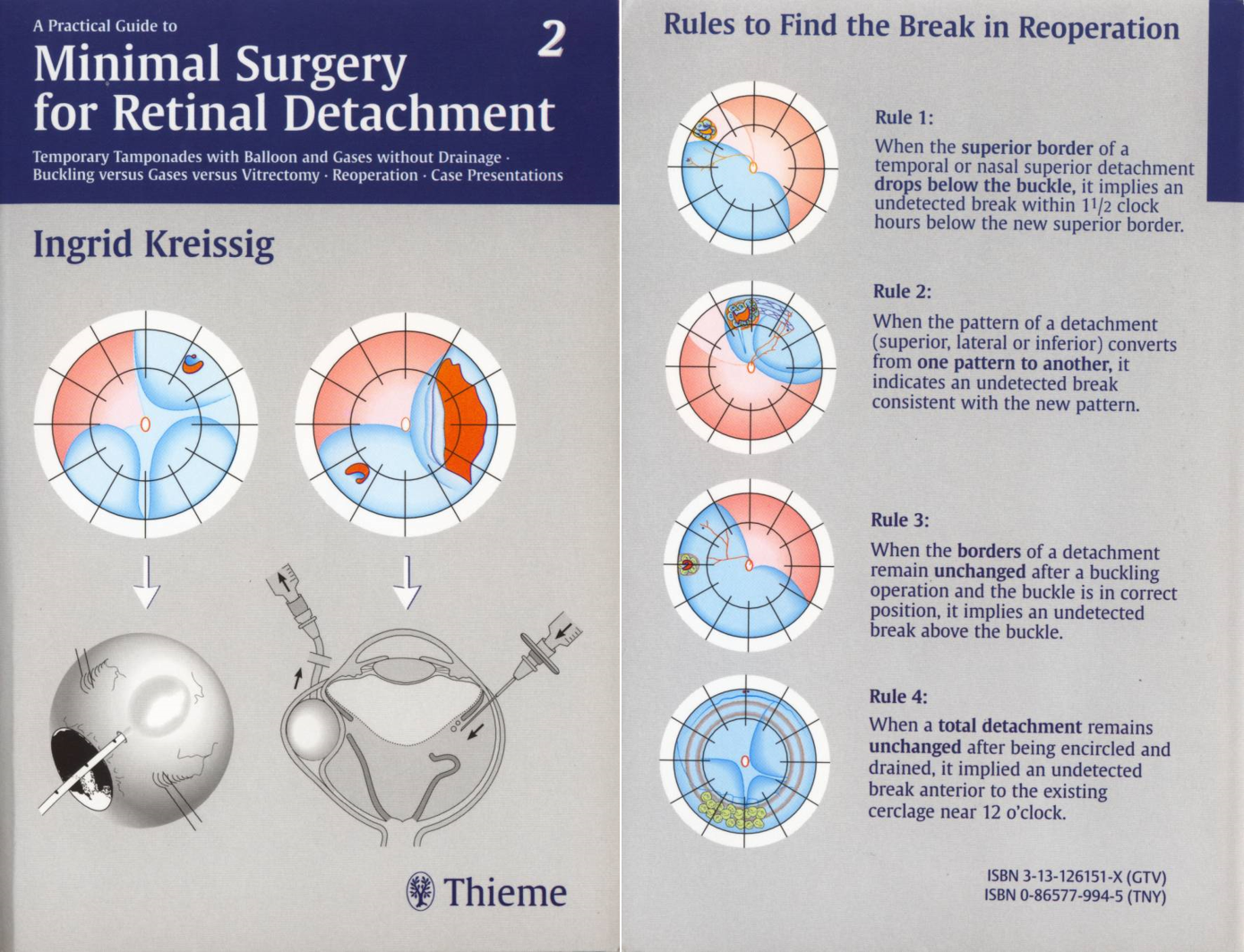
Established original Lincoff’s rules, “Finding the Retinal Hole,” patterns of retinal detachment, which facilitated minimally invasive surgical techniques (with Richard Gieser) (See Figure 1 Below)
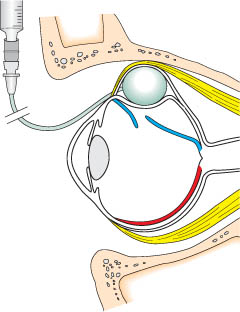
Figure 4: Lincoff-Kreissig balloon insertion Sagittal section of the orbit showing the balloon in Tenon’s capsule shortly after insertion. The balloon is compressed (it has a slightly oval shape) between the globe and the bony orbit. The intraocular pressure is increased.
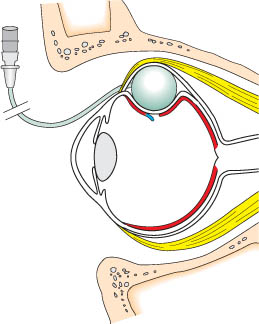
Figure 5: Lincoff-Kreissig balloon effect Sagittal section of the orbit showing the balloon in Tenon’s space after the eye has decompressed and the balloon has expanded to a round shape and closed the retinal break. The retina has reattached and the break is read for laser treatment.
Academic Appointment
1956-2006
Professor of Ophthalmology, Weill-Cornell University
Director of Retinal Research, New York Presbyterian Hospital—Weill Cornell Medical Center
Education & Training
Observership: Charles Schepens
Fellowship: Neuro-ophthalmology, David Corgan, Heed Fellow
Residency: New York University Hospital
Medical School: University of Pittsburgh
Undergraduate: Harvard University
Military Service
US Navy, WWII, Battle of Leyte Gulf
Reflections
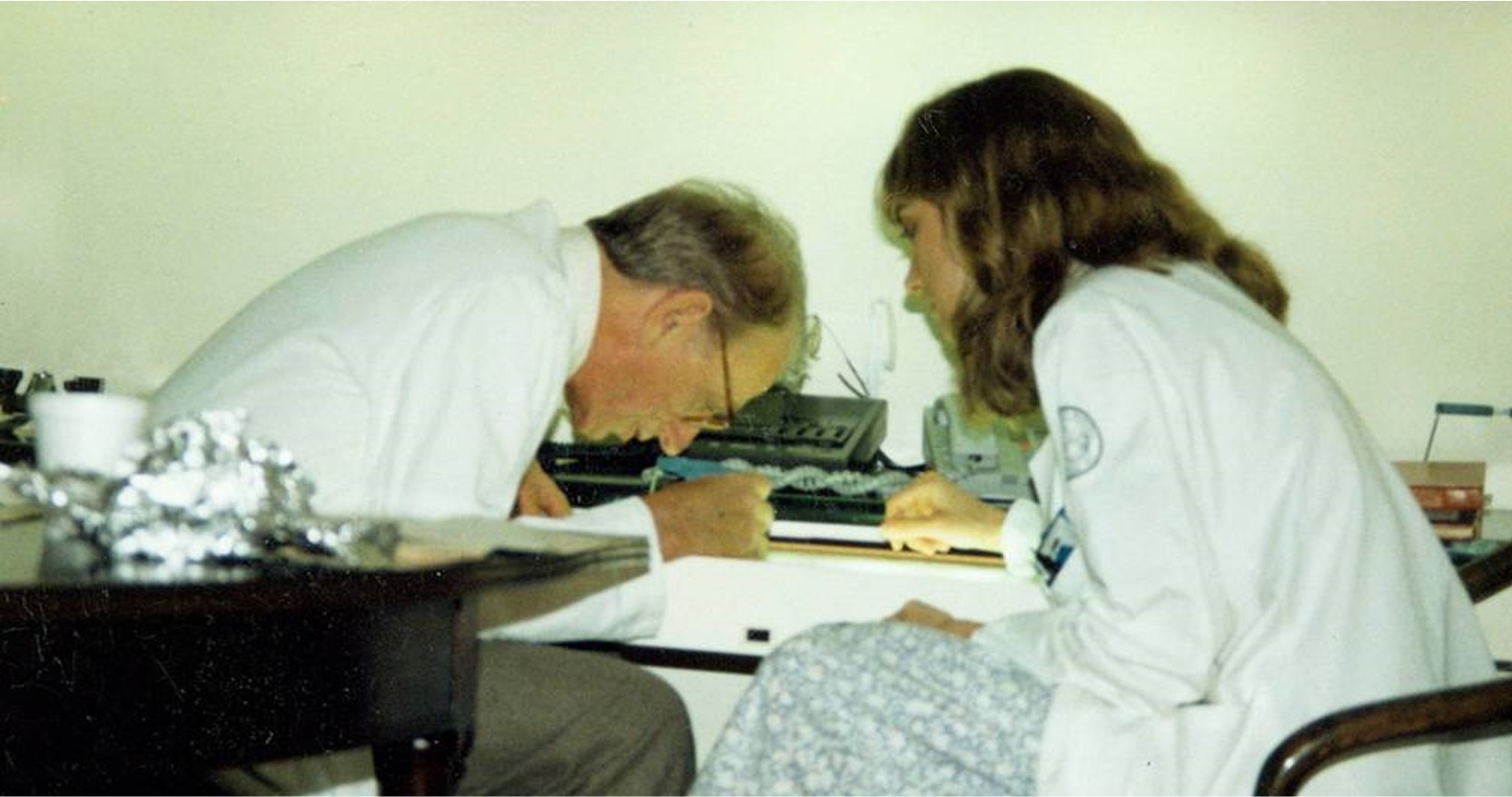
Harvey reviewing slides with Norah at the end of a long clinic. Photo courtesy of Norah Lincoff, MD.
Norah Lincoff, MD (daughter)
When patients and families could not afford a hotel, my father had them stay in his home. He always gave his home number to patients. My father read journals every morning on awakening for 1 to 2 hours. He never stopped; he loved working in his field.
Harvey and Ingrid enjoy the 1994 Club Jules Gonin Meeting in Versailles, France. Photo courtesy Ingrid Kreissig, MD.
Ingrid Kreissig, MD
In 1969, I entered the office, and later the life, of Dr. Harvey Lincoff. I sought him out to learn about his different and new technique for retinal detachment surgery. That’s because as an accomplished detachment surgeon and chief of the detachment department at the University of Bonn, I had started to critically question the results after our maximal surgery for repair of a retinal detachment.
When I first saw Dr. Lincoff, he welcomed me, and questioned me about being a young woman and a retinal surgeon. His first words to me were, “Have you ever done a retinal detachment?” He seemed to be challenging me, but I had to take his comment in stride – I wanted to get to know his retinal detachment surgery technique. Quickly, we realized we had a lot in common, we both wanted to scrutinize traditional facts in surgery, treatment modalities, and science; to practice analytic thinking; and to enjoy challenges. We became friends as well as colleagues.
As we worked closely together, we referred to each other on a first name basis. Harvey was convinced of the rationale and validity of the new Custodis technique, which, however, presented serious postoperative complications. Thus, from 1969-1972, I worked in his lab conducting testing in 312 rabbit eyes to determine the strength of the cryosurgical adhesions, this was done with the intention to replace the necrotizing diathermy of the Custodis technique.
However, this modified non-drainage technique with Harvey’s sponge and cryosurgery was not successful. Why? Harvey concluded that a more rational approach should be established to find the retinal break in a more predictable area of the detachment.
Harvey, together with Dr. Gieser, analyzed 1,000 preoperative retinal drawings and thus defined the well-known Lincoff Rules: How to find the break in a primary detachment. This is one of Harvey’s greatest achievements. In addition, after analyzing the causes of failure after this modified non-drainage technique, Harvey and I realized that we could define an additional 4 Rules: How to find the missed break in an eye that was up for reoperation.
But still, Harvey wanted to eliminate the remaining extraocular and reversible complications after this new non-drainage procedure. After 7 years of experiments, in 1979, the idea of a temporary buckle-without a fixating intrascleral suture came about. However, the biggest problem was, where to find someone to provide a reliable device? Finally, we began working with the Ruesch Company at Stuttgart, and the Lincoff-Kreissig balloon was produced. This balloon operation represents the ultimate minimum of surgical trauma to an eye with a retinal detachment, combined with optimal long-term visual results. This was one of our most important accomplishments in retinal detachment surgery.
My 48-year life partnership with Harvey was exciting, creative, and stimulating. We were able to spend time together on weekends, at meetings and teaching courses around the world. During the transatlantic flights we had time to analyze our work and question the validity of our projects. During these years we shared clinical and research projects on perfluorocarbon gases, radioactive plaques for intraocular tumors, and new treatment modalities. Harvey was always open to new ideas.
On a personal note – Harvey liked to dance, swim, play tennis, sail (he designed a new type of sailboat), he liked parties and spending time with his family, friends, and colleagues. We both were proud of the other and treated each other with respect and admiration. He was modest, witty, tolerant, generous and had a hands-on mentality. Harvey, indeed, was a real “Mensch.”
Now, I thank you, dear Harvey, for the exceptional 48 years we spent together in consideration, enthusiasm, admiration, respect, stimulating creativity and deep love for each other. I do miss him dearly.
Fascinating and entertaining conversations with Dr. Lincoff, Thanksgiving 2010, Buffalo, New York. Photo courtesy Deepa Yoganathan, MD, MSc, FRCS(c), FASRS
Deepa Yoganathan, MD, MSc, FRCS(c), FASRS
Sharing the podium with Harvey Lincoff for the last academic presentation of his lifetime was a highlight of my early career. He was 91 years old at the time, and was so polished, engaging, witty, and humble.
Dr. Lincoff delivered PowerPoint lectures on retinoschisis and ambulatory binocular occlusion. His presentations were filled with precisely detailed, colored retinal drawings—such an important gift to our residents.
He instructed our trainees individually with sketches of Lincoff’s Rules, which, of course, I framed and hung in my office. I can only skim the surface in trying to convey the devotion, achievement, and brilliance embodied by the legendary Harvey Lincoff.
Drs. Stanley Chang and Harvey Lincoff at Dr. Lincoff’s home in 2015. Photo courtesy of Stanley Chang, MD.
Stanley Chang, MD
In 1979, I joined the ophthalmology faculty of the Cornell University Medical College, where D. Jackson Coleman, MD, had just been appointed chairman. Harvey Lincoff was already a world-renowned retina surgeon who was one of the few full-time faculty left from the previous administration.
This was my first position, assistant professor, and I was pleased to be surrounded by 2 colleagues—Lincoff and Coleman—who would serve as excellent mentors. Over the next 16 years, I was fortunate to have been greatly influenced by Harvey’s experience and expertise in retina surgery. While I had been exposed to the finest retina surgeons at Massachusetts Eye and Ear Infirmary (Schepens’ school) and at Bascom Palmer Eye Institute (Norton and Curtin’s school), it was the Lincoff technique that I adapted into my surgical approach to scleral buckling.
Harvey Lincoff was an excellent surgeon who always carefully studied the retina preoperatively to identify all of the retinal breaks and document them with great precision on a retinal drawing. He would often combine indirect ophthalmoscopy with Goldman 3-mirror or QuadrAspheric contact lens. Harvey was an astute observer who was the first to document retinoschisis in optic pit retinal detachments and retinoschisis from diabetic traction.
Whenever I couldn’t find a retinal break, I often would ask Harvey to take a look. It has been written that retinal breaks couldn’t be found in 10% of cases of retinal detachment, but I would say that Harvey was unable to identify breaks in just 1% of patients. Armed with an accurate drawing, he would do a technically perfect operation. Small details such as the intensity and placement of the cryotherapy, suture placement, and non-drainage of subretinal fluid, were not overlooked.
Harvey was also an individual who questioned traditional ideas and always sought to make improvements in retinal surgery. When he discovered the family of perfluorocarbon gases, he asked Dr. Coleman and me to use this gas in vitrectomy cases. It turned out that C3F8 gas, which lasted 3 times longer than SF6, was an ideal one for treating proliferative vitreoretinopathy (1983); this finding later was confirmed by the Silicone Oil Study (1992).
When Harvey was studying the effects of altitude on expansion of gas bubbles and intraocular pressure, he took a rabbit on a chartered airplane to measure the bubble size and intraocular pressure during the ride. His innovations and observations have influenced many principles of retinal surgery that we use today.